
It is easy to damage the mouth during an anaesthetic for a surgical procedure. Retrospective studies depend on identifying problems by looking back on case series or law suits, or by recording complaints, and suggested that the absolute risk of dental injury during operations was low. Prospective studies, which begin before the planned procedure, reveal much higher rates. In one large prospective study, an anaesthetist and a dentist examined over 500 patients before and after an anaesthetic requiring intubation. 25% of the patients had evidence of new dental trauma after their procedure.
The commonest damage were enamel fractures (82 patients, 93 teeth), and eight teeth were avulsed in four patients. Damage was confined to the six first maxillary and mandibular anterior teeth. This study, and other prospective studies, indicate that trauma is far commoner than suggested by the older retrospective studies. The two main risk factors are reported to be difficult intubations, and pre-existing dental status.
Dental damage made up 4% of legal claims against anaesthetists in Italy; 40% in France; 22% in Denmark and 81% of airway management related claims in Norway. The differences probably relate to legal barriers to claims and to exactly what is being counted, but the overwhelming evidence is that dental injuries in surgery are common, and are a frequent cause of legal action. The need for patient safety work on this is obvious.
A Chinese group provide a classic example of a large scale Quality Improvement project intended to increase patient safety by reducing perioperative dental injuries. Sensibly, the improvement team tackled both of the major risk factors, intubation difficulty and dental condition.
In their first, initiation, phase, they introduced devices that made visualisation of the mouth and airway easier, and they also worked on the dental risk factors. They introduced a standardised dental assessment as part of the pre-operative assessment, undertaken by a dental nurse, or dental resident, and included photographs of unstable teeth in the medical record.
In their second phase, the same assessment was conducted but where there was moderate or severe tooth mobility, the pre-op team were required to consult a dentist. If the problem was discovered in the operating theatre, the surgical team consulted a maxillo-facial surgeon.
Pre-operatively, ‘extraction or wire fixation was performed, or dental protection devices such as impression putty and mouth guards were placed‘. This intervention made a dramatic difference (Figure 1).
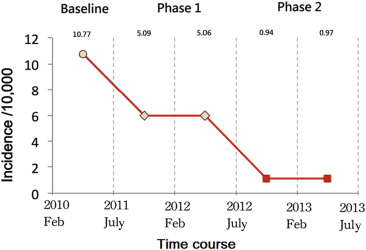
Fig. 1. The incidence of perioperative dental injuries prior to quality improvement program (baseline), initiation (Phase I) and execution (Phase II) Source: Kuo et al., 2016.
In the first phase, improving visualisation and recording dentition produced a substantial drop in injuries. The additional mandated dental interventions in the second phase resulted in a further dramatic reduction.
In Quality Improvement terms, the team identified a significant patient safety problem. After reviewing the risk factors, they sought to reduce the risk related to the method, and also the risk caused by poor dentition. Identifying the problem improved things, but the final action of active intervention by dentists reduced the identified injuries further.
Standard Work is a powerful QI tool. When teams agree how to tackle a problem, and do it consistently, it can make an enormous difference. Clinicians sometimes worry that they will end up with cookie-cutter clinical care. Clinicians are always free to vary their approach if clinically demanded, but having Standard Work gives you a baseline to compare changes against. Standard Work can be thought of as the current best way of doing things: if the team thinks of a better way, tests it out, and it works, they can revise their Standard Work.
This Chinese study gives an insight into the power of linking improvement cycles and revising methods based on your problem analysis. Few dental teams are going to have the time or resource to make changes on this scale, but the method is applicable at any scale of quality improvement work.
Photo by Skip Class: https://www.pexels.com/photo/doctors-performing-a-surgery-13548724/

Leave a comment